
This post originally appeared on Medium.
“It’s easier to fool people than to convince them that they have been fooled.” — Mark Twain
In a recent article entitled “Beware of the Medicaid ‘Big Con’,” Dr. Deane Waldman, director at the conservative Texas Public Policy Foundation, defines the “big con” as follows:
Any good con has three parts: the mark — the one who is conned; the take — what the con man gets; and the fake, the illusion or purposely distortion of reality. The bigger the take, the more marks conned, and the grander the fake, the bigger is the con.
Proposals to block grant and dramatically cut funding to Medicaid would fit the definition of the “big con,” and states should not be made the fool by this scam.
Unfortunately, in the past few years, both House Speaker Paul Ryan and Tom Price, President-elect Trump’s pick to be the Secretary of the Department of Health and Human Services, have proposed block granting the Medicaid program to the states (“the mark”) with the allure that the block grant includes enhanced state flexibility (“the fake”).
Like a fish that bites into the worm without seeing the hook, some governors are duped into falling for the idea that block grants means state flexibility. It does not. If governors are uncertain about that, they should walk over to their state education agency and ask whether the education commissioner and staff there believe education block grants under No Child Left Behind were flexible. All across the country, there has been enormous backlash to the testing mandates that have been imposed on students and schools by federal education block grants.
State leaders sometimes also seem to completely ignore the fact that the federal government would be simultaneously backing away from and shifting the burden and cost of Medicaid to the states. In an analysis of Ryan’s combined Medicaid and Children’s Health Insurance Program (CHIP) block grant in his FY 2014 budget proposal, the Bipartisan Policy Center found that Medicaid and CHIP spending would be $296 billion below baseline in 2022.
To respond to this enormous shortfall, the Congressional Budget Office (CBO) wrote that “states would need to increase their spending on these programs, make considerable cutbacks in them, or both. Cutbacks might involve reduced eligibility for Medicaid and CHIP, coverage of fewer services, lower payments to providers, or increased cost-sharing by beneficiaries — all of which would reduce access to care.“
Children are likely to be disproportionately harmed. According to data from the Kaiser Family Foundation, children account for a majority, or 51 percent, of all Medicaid and CHIP enrollees as of September 2016.
Unfortunately, Vice President-elect Mike Pence doubled down on the so-called “state flexibility” of Medicaid block grants while ignoring the fiscal implications of the cuts on ABC’s This Week on December 4, 2016.
.@mike_pence: “We’re going to keep our promises on Social Security and Medicare,” adds there is “real opportunity” to block grant Medicaid. pic.twitter.com/yDbpsEVxkg
— This Week (@ThisWeekABC) December 4, 2016
In that interview, Pence talked about how his state, Indiana, was given the flexibility to establish Health Savings Accounts (HSAs) under Medicaid and suggests states by given such flexibility “to innovate.” However, what Pence failed to explain is that Indiana was granted that flexibility by the Department of Health and Human Services (HHS) under current law. Indiana doesn’t have to accept a block grant and billions of dollars in funding cuts in order to have program flexibility.
Pence went on to promote repeal of the Affordable Care Act (ACA), but again, he failed to acknowledge that the adults covered by the Medicaid expansion that he touted and supported as governor would lose coverage altogether if the ACA is repealed.
Efforts to block grant and cut Medicaid would be harmful to millions of people, and states should not be fooled into thinking block grants are anything other than that. States must keep their eye and focus on the overriding fact that proponents of block grants want to impose a capped financing structure upon states in order to slash funding to Medicaid and CHIP and that shortfall is a burden that states will be left to address. For example, just like Ryan’s Medicaid-CHIP block grant, Price’s proposed budget would have cut Medicaid and CHIP by an estimated $1 trillion, or by nearly one-quarter, over the next decade under a combined Medicaid and CHIP block grant.
Unfortunately, when I worked for the State of Texas a number of years ago, I observed how some of the nation’s governors are strangely wooed by the allure of “block grants,” despite enormous evidence that they would be harmful to states, the vulnerable people that Medicaid is intended to cover, and the health care system. Even Dr. Waldman, who warned about falling for the “big con,” seems to be susceptible to it. In a blog entitled “Medicaid block grants can work, but there are limitations” in The Hill, Waldman writes that “block grants can work to ameliorate financial and medical care crises in the states but only if the states restore the original intent of Medicaid: state administration.” Unfortunately, Dr. Waldman is in danger of becoming another “mark.”
Medicaid Provides Health Coverage to Low-Income People
First, the original intent of Medicaid was (and still is) to provide a safety net of health insurance coverage to the nation’s low-income children, disabled, and senior citizens through a state-federal partnership.
Fortunately, a number of governors recognize the “big con” for what it is and are not duped by block grants and the offer of state flexibility. In fact, when Ryan proposed his earlier version of a Medicaid block grant, 17 of the nation’s governors wrote a joint letter in opposition to it. The governors explained:
We strongly oppose a congressionally-mandated block grant of federal Medicaid spending, which would shift costs and risks to states. Such a cost shift would severely undercut our ability to provide health care to our residents and adequately pay providers.
As they point out, Medicaid block grants would be a health care disaster. Fortunately, that same recognition helped lead to the defeat of block grant proposals on a bipartisan basis in 1981, 1995, 1996, 2003, and again, in 2005.
Block Grants Fail to Adjust for Changing Need
Second, block grants allow federal lawmakers to bear no responsibility or to provide any assistance with changes in need, such as recessions, natural disaster, or demographic variations that occur over time. States should appreciate that they need extra help during economic recessions, hurricanes, floods, droughts, and changing demographics, but that the federal government would simply walk away from sharing that responsibility under a block grant.
Once again, the governors, who are not fooled by the “big con,” wrote:
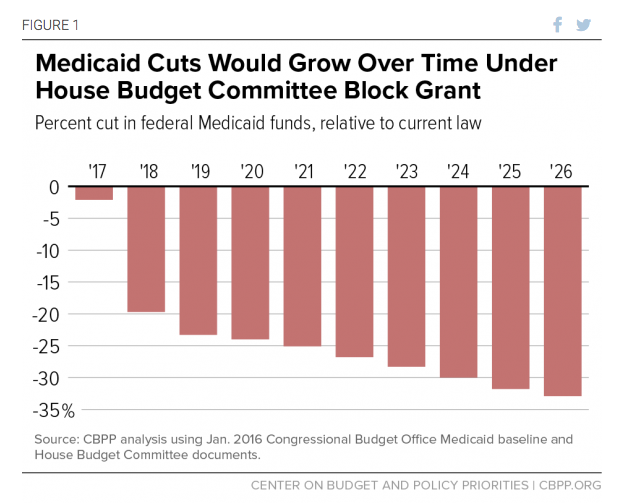
A Medicaid block grant imposed unilaterally by Congress on all states that would cap the federal government’s share of costs and provide annual funding below the projected growth of program costs is simply unacceptable. The inadequacy of funding would grow over time and would be exacerbated by unanticipated increases in health care costs or enrollment. The costs of population increases, aging populations, economic downturns, natural disasters, new diseases or epidemics would all be shouldered by states.
Block Grants Would Shift Costs to States
Third, states should fully appreciate that, through a block grant, the federal government would be abandoning their future Medicaid partnership with states, just as the Baby Boomers are reaching retirement age in record numbers. The Population Reference Bureau estimates that, between 2011 and 2050, the number of senior citizens over the age of 65 will increase from 40 million to 89 million.
This is critically important for Medicaid, as the program paid for an estimated 61 percent of all long-term care expenses in 2012, according to the National Health Policy Forum. To address this demographic tsunami, states will need all the help they can get.
Compounding the problem, just as demand for Medicaid long-term care support will be increasing, public revenues to state and local governments will be declining, as Baby Boomers exit the work force and associated income tax, taxable expenditures, and property taxes decline.
Fortunately, some of the governors are quite aware of the federal abdication of responsibility for the increased costs associated with the retirement of Baby Boomers through Medicaid block grants. As the governors explain:
States would be forced to bear all costs after hitting the annual cap just as the ‘baby boom’ generation is entering their retirement years with a likely steep increase in their health care and long term care costs over the next few decades. The ensuing funding shortfall would leave states with an untenable choice between increasing taxes, cutting other state programs, or cutting eligibility, benefits, or provider payments.
Puerto Rico is Proof that Medicaid Block Grants Do Not Work
Fourth, while there would be a plausible excuse that people could be deceived if Medicaid block grants were something new, the fact is that we have operating, real life examples of how Medicaid block grants would operate. For example, Medicaid funding is allocated by the federal government to U.S. territories, including Puerto Rico, in the form of a block grant. Although it should come as no surprise, these capped allotments are arbitrary, they fail to adjust for need, and they radically underfund the health care services needed by low-income American citizens.
This past February, First Focus sent a letter to the House Energy and Commerce Committee outlining the problems this poses for the children of Puerto Rico. As we pointed out:
The effects on Puerto Rico’s children have been devastating. Doctors are fleeing to the mainland or refusing to accept patients on Medicaid, leaving children without access to pediatric and preventive care. Consequently, children are more likely to have preventable hospitalizations and use overwhelmed hospital emergency departments for illnesses that should be treated by primary care physicians. Furthermore, the lack of access to specialists leaves children at risk of developing preventable chronic diseases.
Consequently, the Medicaid block grant is doing incredible harm to Puerto Rico’s entire health system and is a major factor in the Commonwealth’s debt crisis. Dr. Johnny Rullán, Puerto Rico’s former Secretary of Health and Secretary of the Puerto Rico Healthcare Crisis Coalition, points out:
. . .more than 40 percent of the island’s debt is due to health care and the lack of funding from Medicaid in particular. This chronic underfunding has caused cutbacks in services, a major physician exodus, life-threatening delays in getting appointments and huge delays in payments to hospitals and other medical providers. Patients are suffering and the system is crumbling.
Knowing this, it is unclear why rational state officials could be duped into thinking this is a model of something they would want imposed upon the nation.
Medicaid Block Grants, Coupled with ACA Repeal, Would Be a Disaster
Fifth, if the Congress votes to partially repeal the ACA, the Urban Institute has estimated that the “number of uninsured people would rise from 28.9 million to 58.7 million in 2019, an increase of 29.8 million people (103 percent).” This will place enormous strain on the health care system and state and local governments. In fact, according to the Urban Institute, the newly uninsured would increase uncompensated care by an estimated $1.1 trillion between 2019 and 2028 — a burden that Medicaid would logically be asked to address.
Even worse, if some repeal of the ACA were to be coupled with Medicaid block grants and billions of dollars in cuts, the consequences for our health care system could be disastrous. To address what could be a health system meltdown, federal officials might be gladly willing to give the states “flexibility” to use their “block grants” to:
- Cut off of coverage even more children, pregnant women, people with disabilities, or low-income senior citizens off of coverage;
- Impose enrollment freezes (disproportionately harming babies);
- Place those in need on waiting lists;
- Withhold certain medical benefits, such as mental health or dental coverage;
- Slash payment rates to hospitals, clinics, doctors, dentists, and pharmacies;
- Raise taxes; or most likely,
- All of the above.
In the “big con,” states would be “marks.” But far worse, tens of millions of vulnerable low-income children, people with disabilities, and senior citizens and the health care system itself would also be “marks” or victims of Medicaid block grants. Nobody should be fooled to think otherwise.

Consequently, the states, health providers, and those receiving health services from the program should rise up in unison and oppose the federal imposition of Medicaid block grants.
As the saying goes, “Fool me once, shame on you. Fool me twice, shame on me.”