
EDITOR’S NOTE: This was originally published on Medium.
Real health reform would start with some basic goals and principles, such as: (1) expanding health coverage; (2) reducing costs; (3) increasing access to care; and, (4) improving health quality. Those are four goals that most Americans, regardless of party, would support and actually reflect some of the promises that President Donald Trump made during the campaign and after his election.
For example, in an interview with the Washington Post back in January, President Trump said:
We’re going to have insurance for everybody. There was a philosophy in some circles that if you can’t pay for it, you don’t get it. That’s not going to happen with us. [People covered under the law] can expect to have great health care. It will be in a much simplified form. Much less expensive and much better.
Progress should ensure that fewer people are left uninsured and that health outcomes, access to care, and quality of care are improved. Or, as the very least, health reform should not leave people and our nation’s health system worse off. As such, the children’s advocacy community, the American Medical Association, and others have implored the President and Congress to “do no harm” as they proceed.

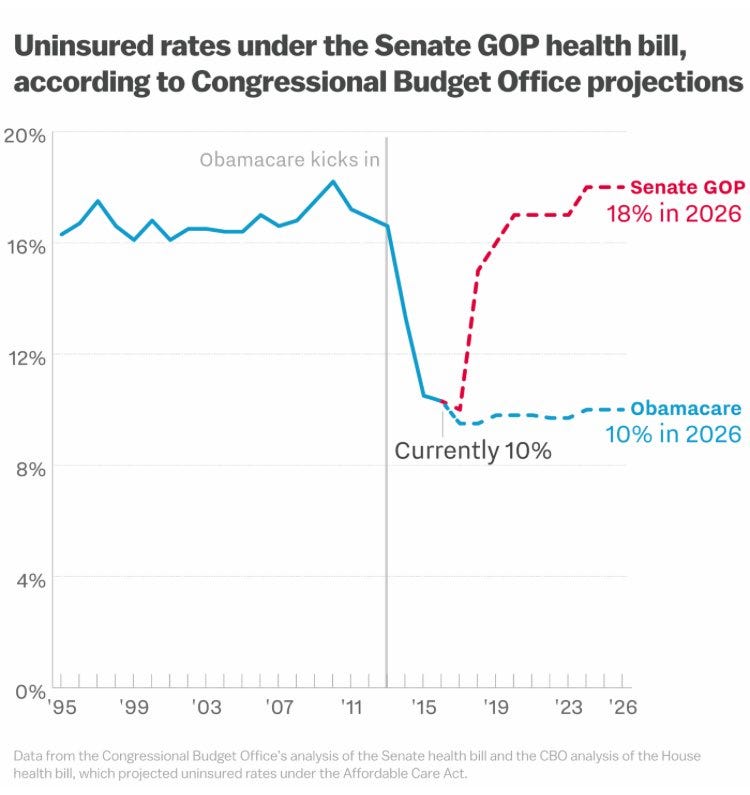
So far, the President and Congress have failed to achieve these basic, fundamental goals, as both the Senate and House bills would increase the number of uninsured by an estimated 22–23 million, raise out-of-pocket costs for may others, and consequently, leave millions worse off in Medicaid, the insurance market, and employer coverage. That will threaten the lives and well-being of Americans across this country and our nation’s health care system.
By definition, this is not progress. It even fails to meet the more simple and fundamental test to “do no harm.” In a previous blog, I highlighted the harm that the House and Senate bills would have on children in foster care. These kids, who have been abused or neglected, deserve much better from us than cuts and rationing of their health care.
Despite the failings of the House and Senate bills, at the very least, one might think that the Republican congressional majorities, who argue they are pro-life, would do no harm to the health of newborns and pregnant women, right?
Indeed, as former House Republican Whip Eric Cantor (R-VA) said before the start of the last Congress in 2015 about the need to prioritize our most vulnerable children:
As the new Congress convenes, I hope the president and members from both parties will keep one number in mind: 8,053,000. That is an estimate of the number of new Americans expected to be born between now and the end of this Congress. . . The future of those 8,053,000 little boys and girls deserve to have the next two years of this Congress focused on them and not the next election.
Moreover, the Republican Party platform includes language claiming to help pregnant women, “We affirm our moral obligation to assist, rather than penalize, women who face an unplanned pregnancy.”
The platform also proclaims, “We are proud to be the party that protects human life and offers real solutions for women.”
Consequently, in recognition of the fact that we have terribly high maternal and infant morality rates in this country, any health care reform effort should include a commitment and solutions to help save the lives of our nation’s mothers and babies.
This would hopefully include their understanding that, as a National Bureau of Economic Research paper showed, the expansion of coverage to pregnant women within Medicaid led to a “reduced incidence of low-birth weight babies” and a “decrease in infant mortality of about 8.5 percent.”
As such, a pro-life and pro-family position for health reform should support protecting the health and financing stability of women who want to bring their pregnancies to term while simultaneously seeking to reduce maternal and infant mortality.
Apparently not.
Trumpcare Shortchanges Medicaid for Pregnant Women and Babies
In fact, Senator Majority Leader Mitch McConnell (R-KY) worked with the 13 Republican men he selected to create a draft bill that would shortchange Medicaid for the costs of caring for pregnant women and newborns and undermine private coverage as well.
According to a Truven Health Analytics study published in January 2013, the cumulative cost of around 4 million annual births in the United States was over $50 billion in 2010. The study found:
· In Medicaid, payments for all maternal care with vaginal and cesarean childbirths were $6,117 and $7,983, respectively.
· Total newborn Medicaid payments were $3,014 for vaginal births and $5,607 for cesarean births.
· In Medicaid, 6 percent of newborns with vaginal deliveries and 14 percent of newborns with cesarean deliveries entered an intensive care unit. The total average allowed payments for newborns that required an intensive care admission were $14,517 for newborns from vaginal childbirths and $20,934 for newborns from cesarean childbirths.
For those with employer-provided commercial insurance, the cost of maternity and newborn care in these same categories was about double the cost of Medicaid. Thus, Medicaid is already quite efficient and frugal in comparison to employer coverage. In fact, many conservatives have complained that Medicaid underpays providers for the cost of delivering health care.
And yet, the President and the Congress are looking to subject the Medicaid program to newly imposed and arbitrary per capita caps that are far below even 2010 spending levels for pregnant women and newborns and would shortchange the states by tens of billions of dollars. Needless to say, this would only exacerbate the problem.
According to Urban Institute estimates, the Medicaid per capita cap in 2017 is estimated to be just $3,352 for adults and $2,002 for children.
It is ludicrous to apply a per capita cap on pregnant women enrolled in Medicaid. On average, Medicaid covers pregnant women for about four months prenatal and two months postpartum or for about six months in total. This effectively reduces the arbitrarily-imposed Medicaid per capita cap in half to an estimated $1,676 per pregnancy, when the cost of maternity care is $7,000 or more. Thus, the Senate bill would only finance one-quarter of the cost of each pregnancy in Medicaid, which could have tragic implications.
In addition, for a newborn’s first full year of life, the average Medicaid per capita cap would also be just $2,002, despite Truven Health Analytics’s studyfinding the average Medicaid cost to be $3,500 for just the first three months of life way back in 2010. Through the full year of life, those costs per baby would be much higher.
In short, the per capita caps are way below the actual costs of having a child and the consequences may be disastrous for mothers, children, and states. Even worse, that shortfall is much greater for medically fragile babies that need care in a neonatal intensive care unit (NICU).
Nickie Korsak of the Michigan March of Dimes explains:
Lack of access and coverage is devastating to the lives and futures of our sickest and most fragile. The debate over lifetime limits, the definition of pre-existing conditions and the funding of Medicaid strikes terror in every parent who has had a baby born premature, ill or with a genetic condition.
Erin Rafferty, mother of Lucia who was born with Aicardi-Goutieres Syndrome, explains how Medicaid was critical to providing her daughter with life-saving treatment in the NICU. Rafferty adds that when her private health plan refused to grant in-home nursing care to children with disabilities that Medicaid provided those critical services. She explains in an article entitled “My Baby Wasn’t Born Healthy and Her Life Still Matters”:
. . .Medicaid steps in to foot the bill. They pay for nurses who administer tube feeding, provide suction and oxygen, and give tens of medications a day, but also nurses who monitor blood oxygen levels and seizures all through the night so parents with special needs can sleep and work and live, too.
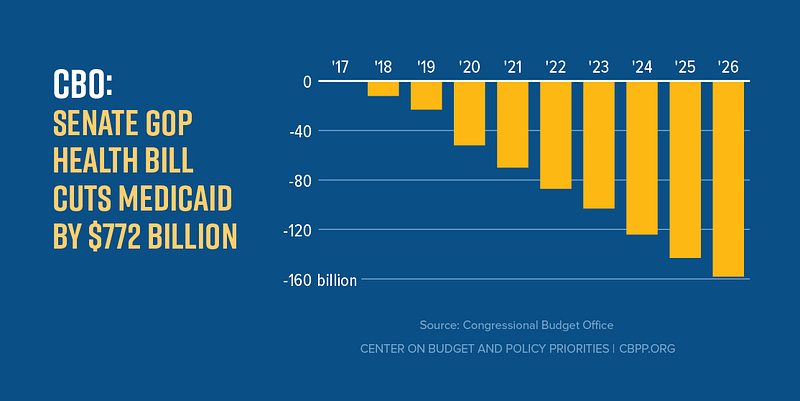
Unfortunately, the Congressional Budget Office (CBO) estimates that the Senate and House bill’s $772–834 billion in Medicaid cuts would lead to 14–15 million people losing Medicaid coverage by 2026 and that millions of others would find their care limited or rationed in a number of ways by the caps and cuts.
Unfortunately, to stay below their federal per capita caps, states would have a financial incentive to impose a litany of rationing techniques to Medicaid, including coverage barriers, cuts to provider payments, benefit limitations, reduced access to care and treatment, and cost shifting to low-income families, who already disproportionately declare bankruptcy in the first year of a child’s life.
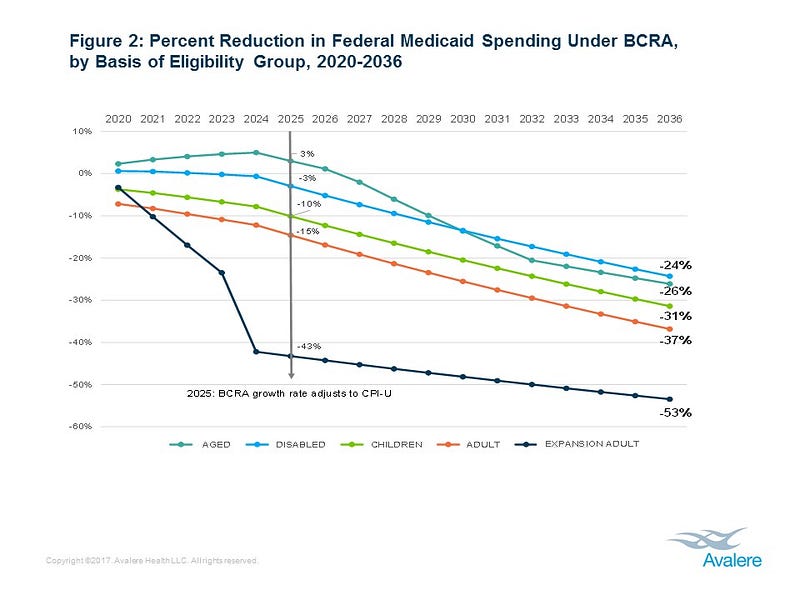
Cuts to pregnant women and children could be particularly severe, as Avalere Health estimates that the percent reduction in federal Medicaid spending under the Senate bill to be 31 percent for children and 37 percent for adults between 2020 and 2036.
Although we cannot be sure what states will do to try to stay below the federally imposed Medicaid caps, the incentives for states will be to enroll healthier, low-cost individuals and avoid more expensive cases, such as pregnant women and newborns, particularly those with special health care needs.
These days it’s not Lucia’s medical fragility that keeps me up at night. . ., but the fact there her abundant quality of life, provided through Medicaid, is being threatened by this bill.
Cuts Negatively Could Negatively Impact Access and Quality of Care
Medicaid per capita caps will hinder the ability of states to ensure that moms and babies have quality health care throughout the pregnancy, birth, and postpartum period. In fact, if you shortchange close to half of all the births across this country, there will be negatively ramifications for our nation’s health system for mothers and babies.
States experiencing an epidemic, such as Zika, would absorb 100 percent of the responsibility of those added costs for its Medicaid patients. Likely, if there are system changes or scientific breakthroughs that create new treatments, therapies, or cures that would improve the quality of care or cut maternal or child mortality, a Medicaid per capita cap or block grant would create a financial incentive for states to restrict or limit access to these added potentially life-saving expenses.
That is not progress, particularly for a nation that already fails to care enough to combat the terrible tragedies of infant and maternal mortality in this country. For example, with respect to maternal mortality, advocates from across the country have been urging states to adopt an initiative in California that is called the California Maternal Quality Care Collaborative (CMQCC).
This effort and focus on women’s health has successfully cut California’s maternal mortality rate to just one-third of that of the American average (7.3 maternal deaths per 100,000 live births compared to 22.0). It requires dedicated resources and a focused dedication to reducing maternal mortality. Medicaid caps and cuts create disincentives for states to make such critical investments.
As an example of what this might look like, Vox’s Julia Belloz points to Texas:
For a preview of what this could do to women’s health, look to Texas, which has the highest maternal mortality rate in the developed world. There, 36 moms die per 100,000 births, or five times California’s maternal mortality rate. Texas has also closed down Planned Parenthood clinics and rejected Medicaid expansion — changes the GOP would like to see ripple across the US. The state boasts the largest uninsured population in America.
Trumpcare Fails to Maintain Key Consumer Protections for Pregnant Women and Babies
Compounding the Medicaid cuts, the bill would make it more difficult to access maternity care, reproductive health, and family planning services in employer coverage.
For instance, the House and Senate bills would allow states to seek waivers that allow insurers to drop essential health benefits that were mandated in the Affordable Care Act (ACA), including maternity care and newborn services.
If the Better Care Act passes, it could mean we could turn back to a time before the Affordable Care Act, when some 88 percent of plans on the individual market did not provide maternity coverage.
Unfortunately, with far too many congressmen, this is purposeful. In an exchange between Reps. Mike Doyle (D-PA) and John Skimkus (R-IL) during consideration of the House bill, Skimkus questioned why men should have to pay for prenatal care.
Nancy Metcalf with Consumer Reports provided an answer to such questions:
So, as a middle-aged childless man you resent having to pay for maternity care or kids’ dental care. Shouldn’t turnabout be fair play? Shouldn’t pregnant women and kids be able to say, “Fine, but in that case why should we have to pay for your Viagra, or prostate cancer tests, or the heart attack and high blood pressure you are many times more likely to suffer from than we are?” Once you start down that road, it’s hard to know where to stop. If you slice and dice risks, eventually you don’t have a risk pool at all, and the whole idea of insurance falls apart.
Metcalf adds:
There’s another reason we know that buying insurance a la carte doesn’t work: we’ve already tried it with maternity care. Before the new health law took effect, insurers can and did exclude maternity coverage from individual plans. In fact, in half of states you can’t purchase maternity coverage on the individual market for any price. In most of the rest, you can buy a maternity rider on your policy. In many cases it costs more than the main policy itself, and you can’t use it for at least a year after you buy it, and it often has a separate deductible of up to $5,000. . .
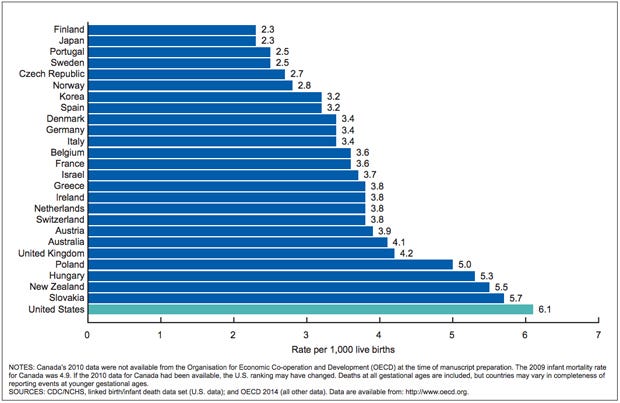
Also, presumably at some point you, yourself, were born. Would it have been ok for your mother not to have insurance for childbirth, which can cost as much as $30,000 for an uncomplicated delivery? The U.S. already has the highest infant mortality rate of any rich industrial democracy. Do you think it’s good for society for some families not to have access to proper prenatal care?
The Senate bill also threatens protections for consumers with pre-existing conditions and those that would be harmed by the reestablishment of lifetime or annual limits.
One area where Trumpcare could have improved coverage for dependents, most often women and children, would be for the House and Senate bills to fix a problem in Obamacare that is referred to as the “family glitch.” Eligibility for the tax credits under Obamacare are based upon both income and whether a family has access to “affordable” employer-based insurance coverage. A Health Affairs brief points out:
The problem is that the definition of “affordable” — for both an individual employee and a family — is based only on the cost of individual-only coverage and does not take into consideration the often significantly higher cost of a family plan. . .
Families caught up in this glitch. . .cannot qualify for premium tax credits to reduce the cost of a Marketplace plan or for cost-sharing reductions to lower their out-of-pocket payments for health services, even if the family cannot afford coverage otherwise.
Trumpcare could have fixed this “glitch” for dependent coverage, but instead, both the House and Senate bills make the problem worse. As Sara Rosenbaum and Tim Jost explain:
Individuals eligible for employer coverage would be ineligible for premium tax credits regardless of the affordability of the employer coverage. This would substantially broaden that ACA’s “family glitch.”
Unfortunately, across-the-board, the Trumpcare bills fail the fundamental principle to “do no harm,” even though Kellyanne Conway promised to do so on MSNBC’s “Morning Joe” when she said:
We don’t want anyone who currently has insurance to not have insurance. Also, we are very aware that the public likes coverage for pre-existing conditions.
Department of Health and Human Services Secretary Tom Price promised even more in an interview on NBC’s “Meet the Press” in March. On that program, Secretary Price said, “I firmly believe that nobody will be worse off financially in the process that we’re going through. . . .”
Moreover, Price defined success as having a system where “more people covered than are covered right now. . . .”
HHS Secretary Tom Price says the new healthcare bill aims to increase the number of people covered. #MTP pic.twitter.com/EmfsbEcdI6
— Meet the Press (@MeetThePress) March 12, 2017
Sen. Bill Cassidy (R-LA) added that any legislation should also meet another fundamental test. As a guest on Jimmy Kimmel Live!, Cassidy responded to a monologue in which Jimmy Kimmel detailed the life-threatening health condition that his newborn son Billy recently faced. As Kimmel said:
If your baby is going to die and it doesn’t have to, it shouldn’t matter how much money you make. . . And no parent should ever have to decide if they can afford to save their child’s life.
In response, Cassidy said:
As you present that, I ask, ‘Does it pass the Jimmy Kimmel test?’ Will the child born with congenital heart disease be able to get everything she or he would need in that first year of life? I want it to pass the Jimmy Kimmel test.
It doesn’t, and it isn’t even close.
According to Stacey D. Stewart, president of the March of Dimes:
. . .the Senate bill makes no investment in promoting maternal and child health or in seeing to it that moms and infants can get the quality care they need for healthy pregnancies and a strong start in life. And if families lose their health insurance, they might not be able to pay for vital care that could save their baby’s life — in the NICU and beyond.
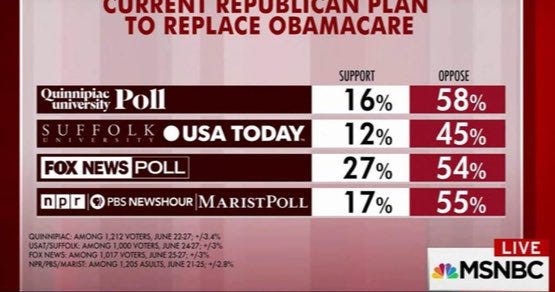
Both the House and Senate bills leave our nation’s pregnant women and babies worse off. Consequently, Congress should follow the American public’s lead and soundly reject these bills. Our nation’s most fragile babies and their moms deserve better — much, much better. These lives and well-being are at stake.
As Rafferty (Lucia’s mother) says:
Let’s preserve Medicaid assistance for people in need because it’s the right thing — the human thing to do. Without it, many people, like my daughter, my family, millions of families will needlessly suffer. Let’s not make health a precondition for humanity: my baby wasn’t born healthy, but she’s worthy of this fight.
Call your U.S. senators today at 202–224–3121 and urge them to reject Trumpcare and to begin working on a bipartisan bill that would improve our nation’s health care system and not leave people worse off.