
Earlier this month, POLITICO reported that, after Congress rejected efforts to cut and block grant the Medicaid program in 2017, the Trump Administration is exploring ways to “bypass Congress” to impose “spending limits” upon the Medicaid program through some form of a block grant coupled with “flexibility.” This threatens the gains and progress that have been made in recent years toward the goal of reducing the number of uninsured people in this country.
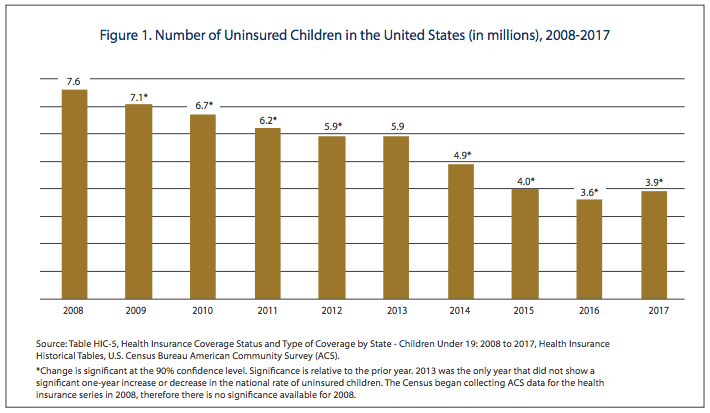
Medicaid, in partnership with the Children’s Health Insurance Program (CHIP), has led the way in helping to cut the nation’s uninsured rate dramatically. This has been a long journey in which the percentage of uninsured children has dropped from 14.9 percent in 1997 to 5.0 percent in 2017 — a reduction by two-thirds over the last two decades. That is the definition of success, although progress has stalled in the last few years.
Further headway has also been made in terms of reducing the number of uninsured adults in recent years due to passage of the Affordable Care Act (ACA) or Obamacare. The Kaiser Family Foundation reports:
The number of uninsured nonelderly Americans decreased from over 44 million in 2013 (the year before the major coverage provisions went into effect) to just below 27 million in 2016. However, in 2017, the number of uninsured people increased by nearly 700,000 people, the first increase since implementation of the ACA.
Despite the progress that has been made, there are still 28 million uninsured Americans, including four million uninsured children that lack health coverage. Furthermore, recent efforts to undermine the ACA and Medicaid and failure to properly extend CHIP on a timely basis have caused the uninsured rate to rise slightly. This is unacceptable and, consequently, the President, Congress, governors, and state legislators should all commit to taking action that recommits the country toward progress.
For example, in the last election, voters in states across the country elected a number of political leaders or passed referendums to expand Medicaid and reduce the number of uninsured people in this country.
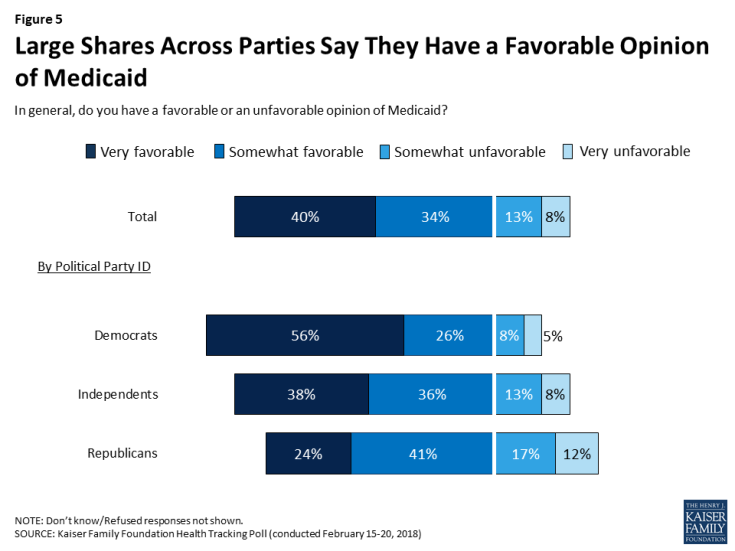
According to polling by the Kaiser Family Foundation, by a 74–21 percent margin, American voters express a favorable opinion of Medicaid.
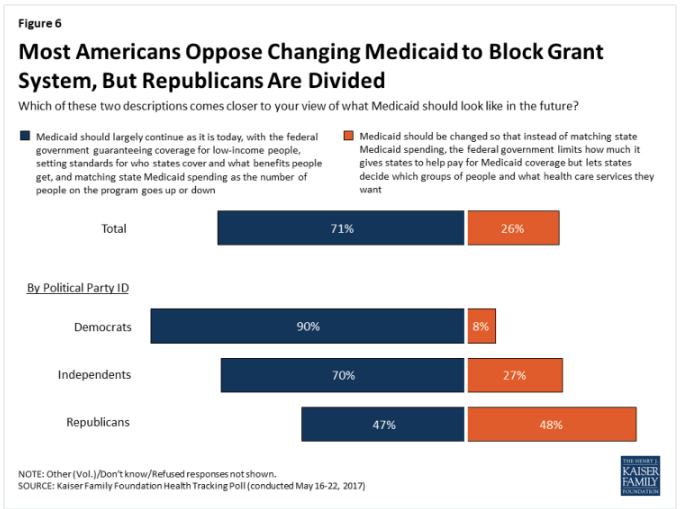
Unfortunately, rather than protecting Medicaid and the coverage it provides, the Trump Administration’s block grant proposal threatens to roll back coverage. The American people oppose this. According to another Kaiser Family Foundation poll, voters oppose block granting and capping the Medicaid program by a margin of 71–26 percent.
Unfortunately, the dreadful idea of block granting the Medicaid program is nothing new. It would be terrible health care policy, but somehow, this zombie idea just won’t die or go away. Sadly, we have seen this idea rise time and time again (in 1981, 1995, 1996, 2003, 2005, and 2017) over the years.
But unlike mythical zombies that cannot really harm us, Medicaid block grants pose an enormous threat to the health and well-being of millions of our nation’s must vulnerable citizens and to our doctors, nurses, hospitals, clinics, and other health care professionals that make up our nation’s health care system. This is why the concept has been repeatedly defeated on a bipartisan basis and should once again.
Under current law, Medicaid is a shared funding responsibility between the federal government and states. When expenses rise, federal and state governments share those costs and they also share in the savings when expenses drop.
By definition, block grants are federally-imposed, arbitrarily-capped limits on funding to states. The federal government unilaterally sets and enforces the cap and effectively steps away from any responsibility for care and services after the arbitrarily capped level is reached.
The following is a list of 10 important reasons as to why Medicaid block grants poses an enormous threat to states, health care providers, and the health and well-being of millions of senior citizens, people with disability, non-disabled adults, and children.
Block Grants Underfund Health Systems: Ask Puerto Rico
First, the history of block grants is that they lead to chronic underfunding of state low-income programs.
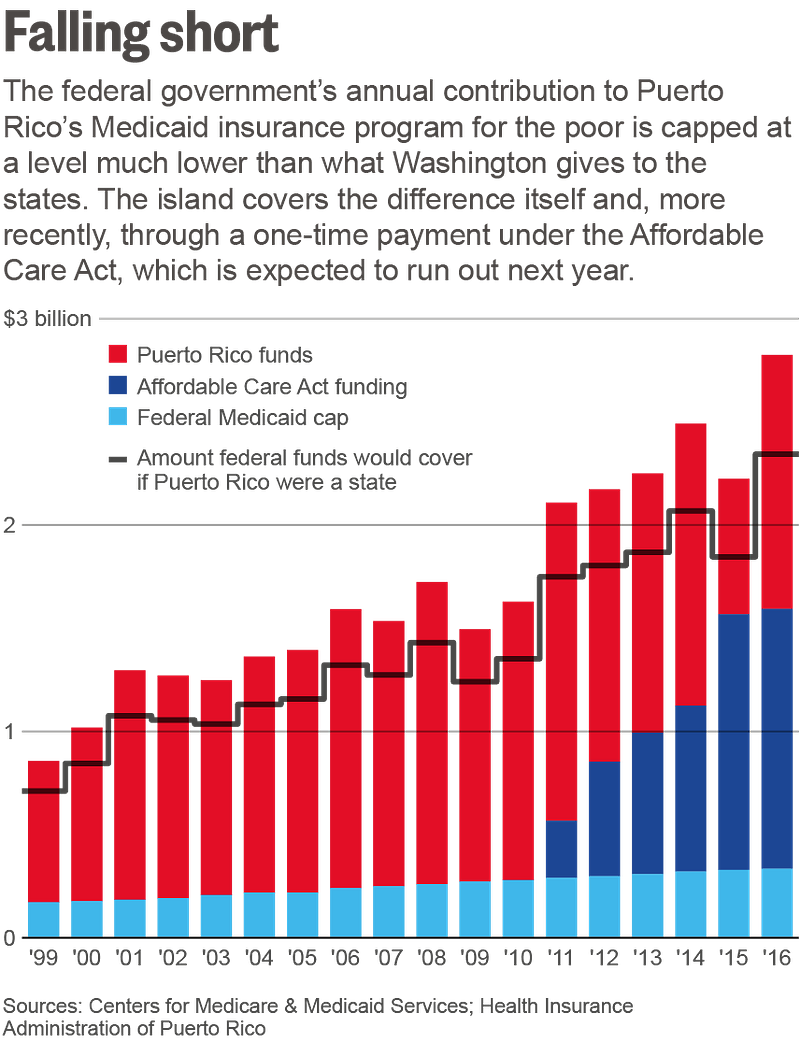
Within Medicaid itself, Puerto Rico’s program has operated under a block grant since 1968. After years of chronic underfunding, a General Accountability Office (GAO) study finds that federal Medicaid funding only accounts for 16 percent of the program’s expenditures.
The shortchanging of Puerto Rico’s Medicaid program under the block grant has consequences has led to a tragic, underfunded, fragile health care system and growing national debt.
Block Grants Fail to Adjust for Natural Disasters
Second, block grants do not adjust for changes in need, such as natural disasters. States would be forced to cut back on care precisely when people are hurting the most.
As Andy Schneider with Georgetown Center for Children and Families explains:
Under block grants, there’s a fixed amount of money, come hell, high water or hurricane.
Block grants compound the disaster, as they significantly limit the federal government’s ability to provide any assistance.
Back In 1995, Sen. Bob Graham (D-FL) explained why hurricanes are a perfect example as to why arbitrary Medicaid caps are unworkable:
. . .when Hurricane Andrew hit south Florida, Mr. President, our Medicaid caseload shot up by 12,000 people. Not only had their homes been blown away, their jobs had been blown away. Therefore, people who had been employed and self-supporting needed the assistance of Medicaid during that time of crisis.
Under block grants, a State that is knocked down to its knees by a flood, earthquake, hurricane, would not find a helping hand from the Federal Government at the time it needed help to get back on its feet. No, Mr. President, acts of God and block grants do not mix.
And yet, sadly, some of today’s policymakers have failed to understand this basic financing problem with block grants.
Block Grants Fail to Adjust for Economic Recessions
Third, Medicaid is something we all pay in to and provides much needed insurance coverage for families and children who either do not have access to private health coverage, are underinsured, or that lose care during economic recessions. When states are hit with an economic downturn, they simultaneously are hit with increased needs and a declining revenue base. Fortunately, through Medicaid, the federal government acts as a critical and immediate fiscal partner to help mitigate potential harm to states and people in need of health coverage.
In sharp contrast, under a block grant, that partnership is broken. Federal funding is capped and so states and low-income populations would be left facing the full brunt of economic calamities and crises with possibly no federal financial support.
Again, Medicaid block grants would compound the harm of an economic recession and result in significant increases in the number of uninsured Americans.
Block Grants Fail to Adjust for Demographic Changes
Fourth, when block grants are established, the base year of funding is typically established based on looking at historical spending for the program in individual states. Block grants can be flat funded, as the Temporary Assistance for Needy Families (TANF) has been since 1996, or it can include some inflation adjusted growth rate, which is often set artificially low by the federal government in order to save money for itself and to shift the fiscal burden over time to the states. Adjusting for inflation and population, the value of TANF grants to states have dropped by 44 percent since it was converted into a block grant two decades ago.
For those states experiencing faster than average overall population growth, including Texas, California, Florida, Nevada, Arizona, Utah, Colorado, Wyoming, Idaho, North Carolina, South Carolina, Washington, Virginia, and Georgia, a block grant would be particularly detrimental. Again, block grants typically fail to adjust for need or growth.
Likewise, it should come as no surprise to states that the federal government is considering moving to capping its federal assistance to states right when the population of senior citizens is increasing. The Population Reference Bureau estimates that, between 2011 and 2050, the number of senior citizens over the age of 65 will increase from 40 million to 89 million.
For those states with rapid growth in their population of senior citizens, a block grant would be particularly problematic, since it would end the federal government’s exposure and partnership for costs associated with services such as high-cost nursing home care just as the demographic tsunami hits. States would be left on their own and the health of senior citizens would be put at great risk.
Block Grants Fail to Adjust for Public Health Crises
Fifth, for states experiencing a public health care crisis, such as Zika, or growth in other health conditions, such as acute flaccid myelitis (AFM) which leaves children either partially or wholly paralyzed, a capped Medicaid program would be disastrous.
Again, the case of Puerto Rico is instructive. When Zika cases increased in the Commonwealth in 2016, federal officials were desperate to help, but sadly, Puerto Rico’s Medicaid block grant left the U.S. Department of Health and Human Services (HHS) “with few options.” HHS could not provide additional financial support under the block grant.
In sharp contrast, Medicaid funding automatically increased for testing and treatment expenses when Flint, Michigan, identified a sharp upturn in the amount of lead in its drinking water. Furthermore, HHS was able to approve of a waiver request from the State to expand Medicaid coverage to reach all affected children.
Neither of these things could have happened under a block grant.
Block Grants Fail to Adjust for Costs Associated with Medical Breakthroughs or Cures
Sixth, in 2016, Congress passed the 21st Century Cures Act. After the passage of the legislation, former House Energy and Commerce Committee Chairman Greg Walden (R-OR) issued a statement that reads:
Of the 10,000 known diseases in the world (7,000 of which are considered rare), there are treatments for only about 500 of them. Yet, the cost and time associated with conducting clinical trials are at all-time highs (it takes upwards of 15 years to bring a new drug to the market, and the cost of developing new drugs has doubled since the early 1980s). This bill would boost medical research and streamline the approval process for new treatments to help accelerate the discovery, development, and delivery of cures.
Meanwhile, despite the Trump Administration’s budget proposal to slash funding to the National Institutes for Health (NIH) by 20 percent, Congress took the opposite approach and funded a $3 billion increase to NIH in FY 2018 and another $2 billion increase in FY 2019. These increases included substantial investment in Alzheimer’s and cancer research.
If these congressional efforts are successful, new therapies and drugs will be developed to improve the lives of the American people.
In fact, a statement by the Food and Drug Administration (FDA) this past week anticipates more than 200 new investigational new drug (IND) applications per year by 2020 and that the FDA will be “approving 10 to 20 cell and gene therapy products a year. . . .”
Clearly, the potential for significant medical advances are high in coming years, but we must expect that they will be associated with some additional costs for the delivery of these potential live-saving treatments and therapies.
This is important to highlight because the federal government may be simultaneously promoting important progress in combatting life-threatening diseases, such as cancer and Alzheimer’s, while walking away from helping low-income children, people with disabilities, and senior citizens from gaining access to these “cures” through the imposition of Medicaid block grants.
Block Grants Will Pit Children Against Other Groups for Funding
The seventh major problem with Medicaid block grants is that, by definition, it would lead to a brutal competition between beneficiaries and among providers over a static amount of money. Nobody would be a winner in such a scenario, but children would likely be among the biggest losers in a world of Medicaid block grants and government rationing.

Kids do not vote, are not part of powerful lobbying coalitions, and do not have Political Action Committees (PACs) advocating on their behalf. In a zero sum game scenario, children are likely to have the least political influence.
As Republican Senator John Chafee said in opposition to Medicaid block grants back in 1996:
As states are forced to ration finite resources under a block grant, governors and legislators would be forced to choose among three very compelling groups of beneficiaries.
Who are they? Children, the elderly, and the disabled. They are the groups that primarily they would have to choose amongst. Unfortunately, I suspect that children would be the ones that would lose out.
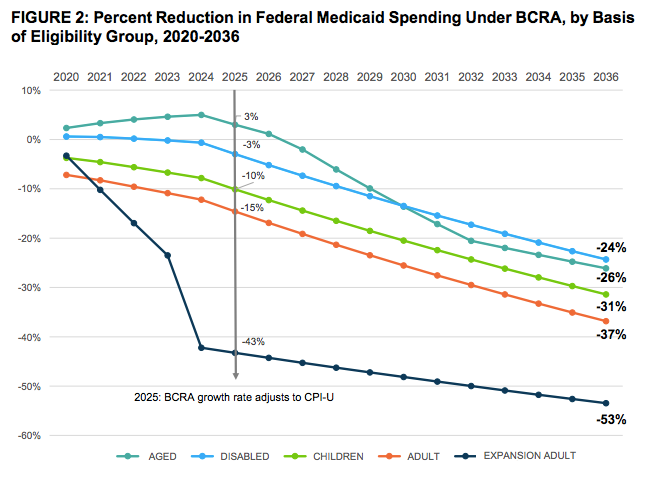
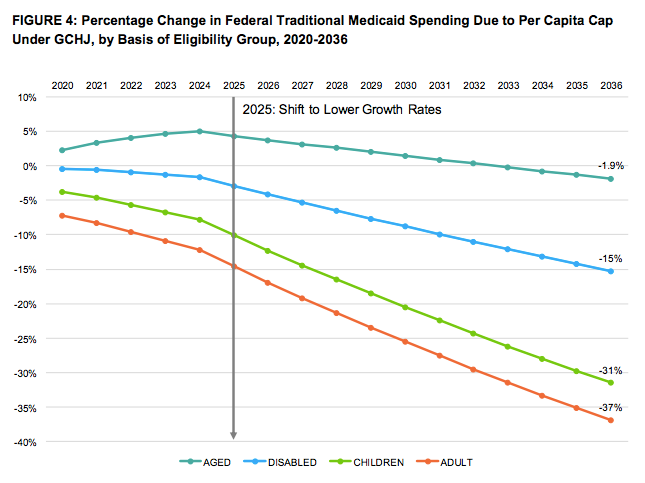
This very scenario played out during the 2017 debate over ending the ACA and capping the Medicaid program. Over the course of the nine-month debate, as groups pushed back against the across-the-board caps, modifications were made by lawmakers having more to do with politics than policy. At the very end of the debate, the final legislative proposal left standing in the Senate was the Graham-Cassidy amendment.
While adjustments were made by Congress to partially mitigate the harm to senior citizens and people with disabilities under the proposed Medicaid caps, the disparity in harm to children became more pronounced over the course of the debate, as these estimates from Avalere Health demonstrate.
Block Grants Will Put Pressure on Other State Programs and Services
Eighth, in any of the scenarios mentioned above, if block grants cause states to have to commit greater resources to provide health coverage to its Medicaid enrollees, it will place greater pressure on everything else that states fund, including public health and education programs. Again, this could be disproportionately harmful to children.
Furthermore, a report prepared by Sasha Pudelski for the American Association of School Administrators (AASA) adds:
If a per capita cap or block grant were to be enacted, school districts would stand to lose much of their funding for Medicaid. A block grant means that districts would no longer receive a dedicated source of funding based on the serves they are reimbursed for providing to students.
This would be particularly harmful to individuals with disabilities and low-income students, but would also likely negatively impact all students. As the report explains:
A Medicaid block grant would mean districts are forced to cut services here they can legally do so (general education) in order to continue meeting the needs of students they must legally prioritize serving (special education students).
Block Grants by Waiver Could Lead to Political Abuse
And finally, although we do not have all the details of how the Trump Administration might seek to pursue this tragic policy, we do know from past proposals that the federal government would arbitrarily set an amount of money that it would cap to states in the future. Under waivers, the federal governments could negotiate with states individually and in ways that could be purely political, particularly since there is no “right” way in which to set such a cap.
With billions of dollars at stake, Trump Administration officials will have enormous leverage with states to make what are rather “political” decisions with funding in both the short- and long-term. They can reward friends and punish enemies with different baselines, different assumptions, different growth rates, and more. As we head into a coming presidential election, this can be particularly troubling.
Block Grants Would Undermine the Guarantee of Coverage
Finally, it must not be forgotten that the original intent of Medicaid was (and still is) to provide a safety net of health insurance coverage to the nation’s low-income children, disabled, and senior citizens through a state-federal partnership.
A block grant undermines that partnership and simply shifts all financial risk to the states under the guise of “state flexibility.” As any or all of the situations aforementioned arise, including economic recessions, natural disasters, population growth, aging populations, public health crises, or medical breakthroughs, states will find themselves without a federal financial partner to help and with nothing more than their newly granted “flexibility” to:
- Reduce eligibility or impose barriers to coverage for low-income children, pregnant women, people with disabilities, non-disabled adults, or senior citizens;
- Impose enrollment freezes (disproportionately harming babies);
- Place those in need on waiting lists;
- Withhold certain medical benefits, such as mental health or dental coverage;
- Slash payment rates to hospitals, clinics, doctors, dentists, and pharmacies;
- Raise taxes; or most likely,
- All of the above.
When Sen. Graham was confronted with House Speaker Newt Gingrich’s (R-GA) proposed Medicaid block grant nearly 24 years ago, he successfully admonished the state leaders to not be fooled by the proposal. Sen. Graham explained:
I have a warning for [governors], or more accurately a proverb for them. The proverb goes as follows: Fish see the worm, not the hook.
Those governors who are salivating, who are so anxious to gobble up block grants being proposed, will feel the hook when their economies stumble, when an epidemic strikes, when a natural disaster hits, when inflation creeps up again, or when their population grows. Worst of all, they will be held accountable in history for killing a program that actually had achieved its objectives and nurtured a national pride in providing basic health care for fragile and vulnerable citizens.
Graham’s words hold just as true today.
Medicaid block grants would unravel decades of progress toward reducing the number of uninsured Americans and fundamentally undermine the nation’s long-standing commitment to guaranteeing health care coverage to millions of vulnerable low-income children, people with disabilities, and senior citizens.
Conclusion
Consequently, Medicaid block grants should be sounded rejected, just as they have been repeatedly in the past. Now is not the time for our nation to retreat from two decades of progress, particularly when it comes to the health and well-being of our nation’s most vulnerable citizens.
As Peter Harbage and Sarah Arnquist explain, “. . .a block grant undermines the long-term investment in America’s greatest asset for future economic growth: our children.” The decisions that are made today will determine their tomorrow.