
Written by Bruce Lesley and Bryan Sperry
In 1996, in the face of a national crisis whereby 1 in 7 children in this country were uninsured, President Clinton and a Republican majority Congress came together to enact the Children’s Health Insurance Program (CHIP).
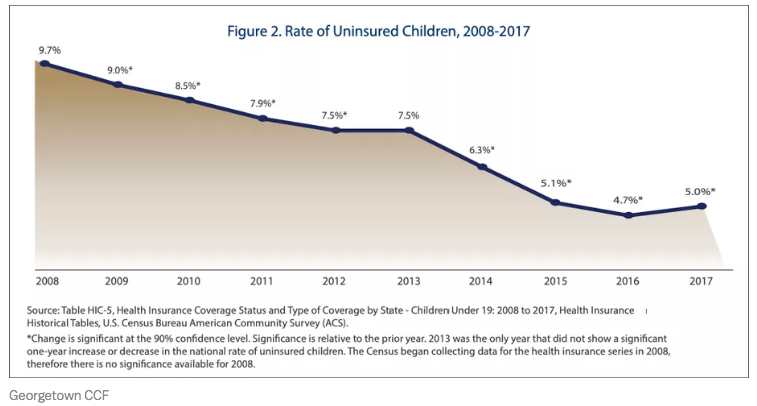
Over the course of the next two decades, the uninsured rate for children has been cut by over two-thirds. Today, 1 in 20 children (or just 5 percent) lack coverage. In tandem with Medicaid, CHIP has proven to be an enormous success story.
Both political parties are debating changes to the health care system. Republican President Donald Trump just released a budget proposal that would slash funding for health care in Medicaid and the Affordable Care Act (ACA) exchanges by $777 billion over 10 years and disproportionately cut funding for child health.
In contrast, Democratic Member of Congress and presidential candidates are crafting various proposals that would seek to expand health coverage through some combination of a single-payer system or expansions of either Medicare or Medicaid.
With respect to proposals that would expand coverage, many simply assume or take for granted that this would undoubtedly be good for children. It could achieve the goal of ensuring that all children have coverage and that would be great.
However, advocates for children are also aware of the potential for harm, as some of these proposals completely repeal present coverage options for millions of children to be replaced with an entirely new system. For obvious reasons, there is some concern with respect to how this would all work, as there is some history with such proposals that is worth recalling. In short, for child advocates, experience tells us that the details of coverage and benefits are critical.
Health Reform Principles for Children
In a joint document laying out some principles of importance to children in these debates, the American Academy of Pediatrics, the Children’s Defense Fund, the Children’s Dental Project, the Children’s Hospital Association, Family Voices, First Focus Campaign for Children, Georgetown Center for Children and Families, the March of Dimes, and the National Association of Pediatric Nurse Practitioners write:
As a nation, we must build on what is working for millions of children, pregnant women and their families by keeping Medicaid and CHIP strong and enrolling all eligible children, strengthening private coverage, and working toward a health care system that meets the needs of ALL children, pregnant women, and their families, regardless of their health or immigration status, family income, or zip code.
Any change to our health care system must further improve coverage for children and pregnant women. They must not lose ground.
Put simply, first, do no harm.

The principles include the following standards:
· All children must have health coverage that provides all medically necessary, age-appropriate benefits to promote healthy child development, and all pregnant women must have coverage for maternity and newborn care.
· All children and pregnant women must have access to health care that is affordable for their families.
· All children must have timely access without administrative barriers to the full range of age-appropriate health care providers, including pediatric and perinatal specialists, sub-specialists, and facilities.
· All children and pregnant women must receive high quality care informed by robust [pediatric-specific and maternity] quality measurement.
· All children and pregnant women must have continuous, consistent coverage with no gaps in care.
In other words, children need affordable pediatric-specific benefits that promote healthy child development, affordable coverage, access to pediatric-focused provider networks, high quality and continuous care.
As the President, presidential candidates, Members of Congress, health reform advocacy groups, and think tanks roll out a variety of health care reform packages in the coming months, they must fully understand that children are not little adults and one-size-fits-all policies often fail our kids.
As Michael Freeman writes in his book The Moral Status of Children:
It is important that all those that formulate policy should be compelled to consider the impact their policies have on children.
Unfortunately, children are often an afterthought in policy debates. We have witnessed the failure to do so time and time again. Freeman adds:
All too rarely is consideration given to what policies. . .do to children. This is all the more the case where the immediate focus of the policy is not children. But even in children’s legislation the unintended or indirect effects of changes are not given the critical attention they demand. . .
But where the policy is not “headlined” children. . ., the impact on the lives of children is all too readily glossed over.
Sadly, this has often been the case with respect to health care policy. In the debate over repeal and replace over the Affordable Care Act (ACA), children were repeatedly ignored. For example, during a repeal vote in 2013, Rep. Steve Scalise (R-LA) offered an amendment that sought to repeal the ACA or Obamacare.
The House passed the budget resolution that included the Scalise amendment to defund Obamacare by a vote of 230–189. Unfortunately, the Scalise amendment, whether intentionally or unintentionally, eliminated funding for CHIP and would have also had a number of other negative impacts on children.
The Department of Health and Human Services Secretary Kathleen Sebelius wrote in an analysis of the Scalise amendment:
Federal funding for the Children’s Health Insurance Program (CHIP) would end on October 1, [2013]. . . The delivery of health care to medically-underserved people at many community health centers would be reduced due to a nearly 60 percent reduction in federal funding. National Health Service Corps funding would be eliminated. The Health Resources and Services Administration’s Maternal, Infant, and Early Childhood Home Visiting program for at-risk children (which encompasses grants to states and Tribal entities) would be eliminated. . . A funding prohibition would also appear to block federal enforcement of all of the health insurance market reforms enacted in the Affordable Care Act, including the prohibition on pre-existing condition exclusions for children, dependent coverage for young adults under age 26, the prohibition of lifetime limits, and coverage of recommended preventive services without cost sharing.
Fortunately, this language was rejected in the Senate, but only after a government shutdown caused by Sen. Ted Cruz’s (R-TX) attempt to demand repeal of the ACA in order to keep the government running.
Four years later, in 2017, little to no attention was given to how ACA “repeal and replace” packages in Congress would impact children. Rep. Jaime Herrera Beutler (R-WA) attempted to offer an amendment that sought to protect children from the Medicaid cuts under the bill, but sadly, the House Rules Committee rejected its consideration.
Subsequently, in an important analysis by the Congressional Budget Office (CBO) as to the impact of the House bill would have on federal spending and coverage levels, the data on coverage was focused on how it would affect coverage on the non-Medicare population. In the charts and analysis that followed, the entire focus was on the legislation’s impact to people ages 18–64.
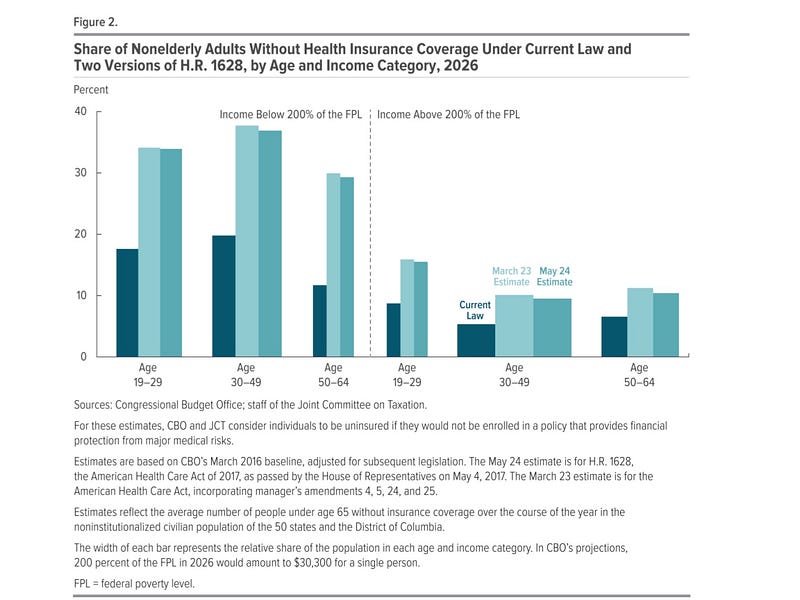
Shockingly, the effect on children, who represent one-quarter of the nation’s population, was completely ignored.
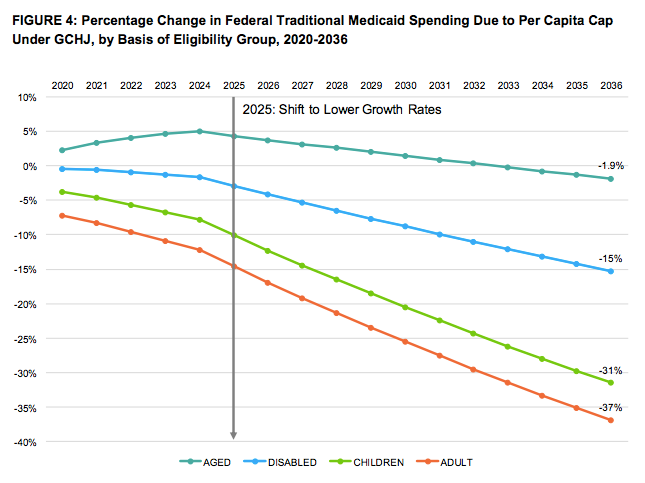
To ascertain how the bills would impact children, the Children’s Hospital Association commissioned a study by Avalere Health. That analysis found the Medicaid cuts in those packages would have disproportionately harmed children. By 2036, the level of Medicaid cuts to children against current law would have been 31 percent compared to 1.9 percent for senior citizens and 15 percent for people with disabilities.
Democrats and progressive advocates should not take solace that these two examples happened during consideration of Republican health reform efforts.
Unfortunately, during consideration of the ACA back in 2009–2010 and just months after having passed an extension of CHIP, the Democratic-led House of Representatives legislation decided to repeal CHIP and move millions of children into the ACA marketplaces. A number of insurers, providers, and progressive organizations supported this change.
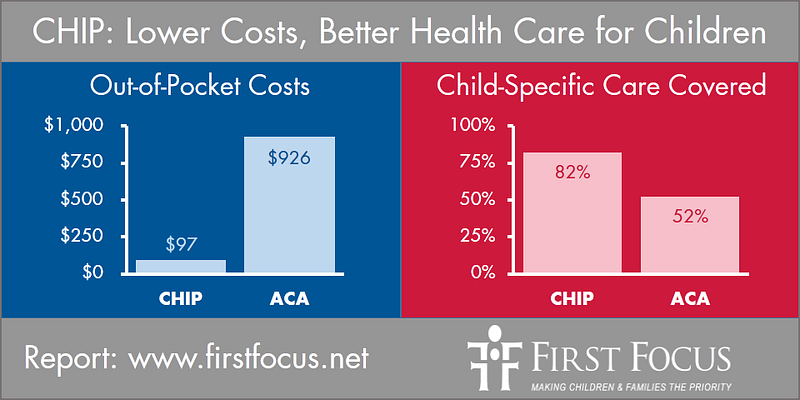
Children’s groups were skeptical and many were certain this would leave kids worse off. The Robert Wood Johnson Foundation commissioned an actuarial value study to compare CHIP to coverage in the ACA marketplaces. In that analysis by Watson Wyatt Worldwide, it was discovered that the 8 million children covered by CHIP would have been left worse off in terms of both benefits and affordability.
In response, an amendment by Sens. Jay Rockefeller (D-WV) successfully protected CHIP from being repealed.
Past as Prologue: The Devil Is in the Details
With that backdrop, it should not be a surprise that child advocates are warily reviewing health reform legislation being proposed now.
Edwin Park at Georgetown Center for Children and Families put together nine important design questions for policymakers developing health reform proposals to consider in order “to further advance the goal of affordable, comprehensive health coverage for all children, while avoiding children inadvertently falling through the cracks and being made worse off.”
Those questions include:
1. How would the coverage expansion proposal affect Medicaid and CHIP coverage of children?
2. Would the new coverage expansion’s benefit package be tailored to children’s unique needs?
3. What would be the premium and cost-sharing requirements under the new coverage expansion?
4. How would the coverage expansion measure and ensure quality of care?
5. What would be the health care delivery system under the coverage expansion and how would health care providers be reimbursed?
6. What are the beneficiary access protections under the coverage expansion?
7. How will the coverage expansion be administered?
8. What is the implementation timeline for the coverage and is there a transition period?
9. How will children’s needs specifically be addressed in any new coverage expansion?
Health Reform Ideas for Children
There is a wide array of health reform proposals being developed or considered on both sides of the aisle. At First Focus Campaign for Children (FFCC), we have proposed the following ideas to improve children’s coverage in our Proactive Kids Agenda for the 116th Congress:
1. Make CHIP permanent and eliminate the CHIP funding cliff;
2. Create a system so that all children eligible for Medicaid and CHIP have continuous coverage from birth through age 5;
3. Permit families to buy-in to coverage through Medicaid or the Federal Employees Health Benefits Program (FEHBP);
4. Improve the ACA by improving affordability, fixing the “family glitch,” and, repealing the “Cadillac tax”; and,
5. Enact the Health Equity and Accountability Act (HEEA) to improve the health, equity, and well-being of all families, including immigrants, across the nation.
These ideas all build upon and improve our health system to promote a good start in life, the growth and development of children, and improved equity. With 95 percent of children in the United States with health insurance, now is not the time to go backwards by throwing away the proven child-friendly CHIP and Medicaid programs.

For Children, What Is ‘Medicare for All’ After All?
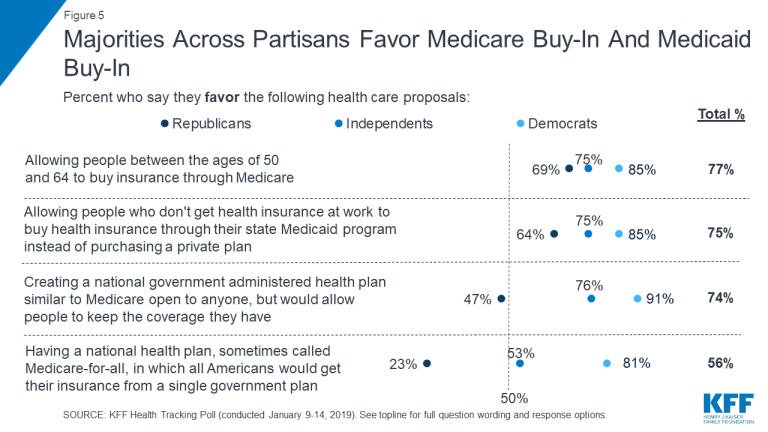
Beyond these ideas, there is a growing conversation about a variety of “Medicare for All” proposals. Some of these proposals would live up to the name “Medicare for All” by expanding the program in various ways to enable everybody to be enrolled through it.
Others are proposing the creation of a new Medicare buy-in option for certain categories of people, such as people over the age of 50, or to create a Medicare-like option on the ACA marketplaces in order to expand health coverage.
And still other proposals are called “Medicare for All” but are actually not about Medicare at all. In fact, the premise of this approach is to blow up the entire health care system, including Medicare, and move people to an entirely new single payer system.
Consequently, there is great irony that some advocates and the media are saying that policymakers supporting “universal coverage” are vague but somehow feel being supportive of “Medicare for All” is not. The various Medicare approaches are radically different and all raise very different challenges for children.
The first “Medicare for All” approach calls for moving millions of children out of Medicaid and CHIP into the Medicare program. Since Medicaid and CHIP were created with children in mind and have pediatric benefits, pediatric networks, and strong affordability provisions, this approach leaves child advocates with numerous questions as to how those protections and standards will be established and guaranteed in a new Medicare system.
The second set of proposals involves giving people options to buy into Medicare. For example, one proposal would create a Medicare buy-in for anyone over the age of 50. This approach would obviously not affect children at all, but leave children without an expansion of coverage. Another proposal would create a buy-in option through Medicaid.
The last set of “Medicare for All” proposals would actually repeal Medicare, Medicaid, CHIP, and private health insurance coverage options for children and other populations and move them to an entirely new health care or single payer system.
While some progressive health reform advocates and the media are criticizing those that do not sign up for this approach as being vague or not bold, we would argue the opposite. In fact, the truth is that this approach is the one most lacking in the way of details.
For example, H.R. 1384, the Medicare For All Act of 2019, repeals both Medicaid (Title XIX) and CHIP (Title XXI) coverage for millions of children.

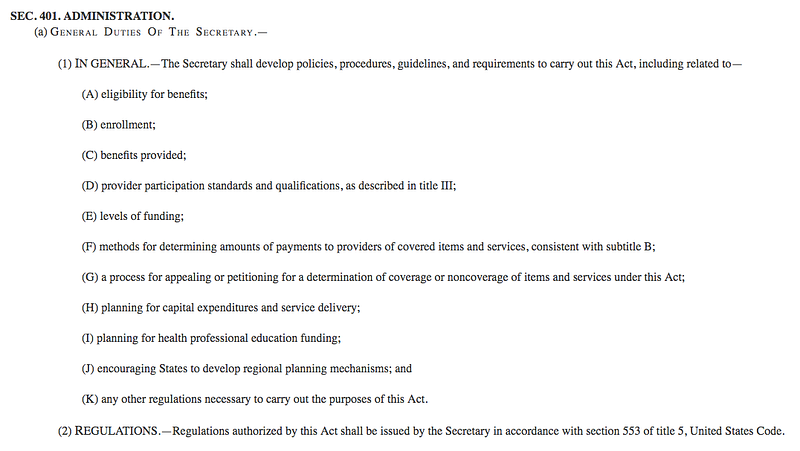
In its place, standards and protections under the new health system are both vague and often left up to “the Secretary” to establish.
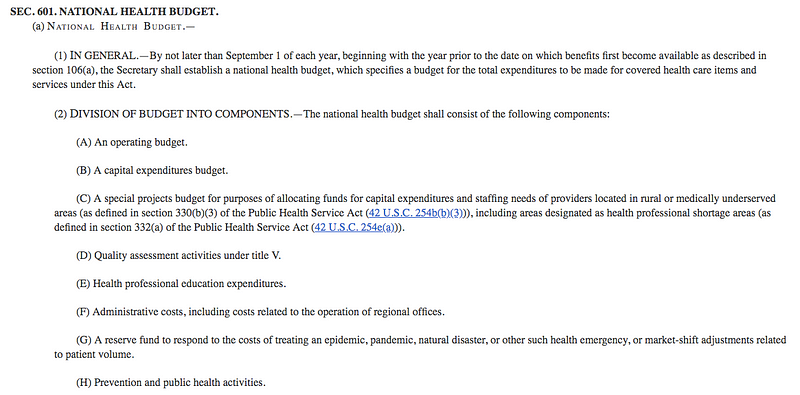
Like many health reform and progressive advocates, child advocates have long been opposed to arbitrary caps on program spending, such as Medicaid block grants or per capita caps. Unfortunately, H.R. 1384 includes language that imposes a global budget or global cap on spending that is, yet again, set by “the Secretary” or by Congress.
Literally, for decades, child advocates have repeatedly fought proposals to establish arbitrary limits, such as Medicaid block grants or per capita caps, and now are being asked to support that very approach for our entire health care system.
While Canada has a system of global caps in its health care system, another example for consideration is Puerto Rico’s block granted health care system. That has been an outright disaster and may continue to cause many Puerto Ricans to flee the Commonwealth for the mainland. We should eliminate that cap rather than impose one on the nation.
Before we are willing to endorse a “Medicare For All” health reform proposal, we must have answers and the confidence to ensure the changes will work for children, with standards and protections in place so children would not be left worse off. It is not acceptable to gamble with the health of children.
Therefore, to all our single payer activist friends, it really is not the Democratic presidential candidates or other advocates that should have to justify their positions to you at this moment in time. The onus is really on you.
If you wholeheartedly believe in this approach, you need to demonstrate to the country how repealing Medicare, Medicaid, CHIP, and private health coverage and placing all people into an entirely new system with global caps is not going to leave people worse off. It won’t be easy.
Oh, and please don’t forget the children.
Bryan Sperry’s career in health care in Texas includes service in Texas government as a special assistant for the Lt. Governor, director of a task force on indigent health care, administrator of Medicaid programs for children and founding director of the state’s center for rural health. He served as president of the Children’s Hospital Association of Texas and was a founding member of the Texas CHIP coalition. He has been honored by the Texas Pediatric Society and Texans Care for Children for his advocacy on child health.