
Congress is proposing devastating cuts to Medicaid, and once again, children are directly in the crosshairs.
The latest budget proposal from the House of Representatives includes up to $880 billion in cuts to Medicaid – a staggering number aimed at partially offsetting $4.5 trillion in tax cuts primarily benefitting corporations and the wealthiest people in society like Elon Musk.
Budgets are about priorities. Sadly, the House is looking to prioritize tax cuts for the rich by rationing and denying health care to children.
At a level of $880 billion in Medicaid cuts over 10 years, the House would gut Medicaid’s federal-state matching partnership and replace it with a per capita cap system in which the federal government would arbitrarily cap the amount of money per individual, regardless of actual costs.
On paper, a per capita cap might sound like a simple budgetary adjustment. But in reality, it forces states to ration care, slash benefits, reduce provider payments, and make impossible choices about which children, senior citizens, people with disabilities, and low-income adults get health care and which do not.

The whole point of this budget-cutting exercise is to arbitrarily cut, cap, and limit federal funding for health care – which would Make America Uninsured, Underinsured, and Unhealthy Again.
The per capita cap would be imposed – typically by capping payments per person below medical inflation – to achieve some arbitrary budget target of “savings”. This would be like deciding to only partially put a roof on your house and then acting surprised when the house floods after it rains and when the ceiling eventually caves in.
Health care access saves lives and money in both the short- and long-term. Neglecting and rationing the health of a child leads to bigger, costlier problems over a lifetime.
The Per Capita Cap – What It Is and Why It’s Dangerous
Under current law, Medicaid’s sharing financial partnership makes it responsive to changing needs and adjusts to meet an array of conditions, including rising health care costs, economic downturns, natural disasters, epidemics, medical advances, and changing demographics, such as the aging of the population. Medicaid spending rises when there is a crisis and declines when need drops.
A per capita cap destroys this model, locking in an arbitrary spending limit per person that does not adjust to real-world medical needs and economic changes.
Per capita caps would leave states with the task of slashing coverage, benefits, or services to people who rely on Medicaid or cutting payments to doctors, hospitals, and other health care professionals to care for senior citizens, people with disabilities, children, pregnant women, and other low-income adults.
Under a per capita cap:
- The federal government sets a fixed amount per Medicaid enrollee rather than covering a percentage of states’ actual costs.
- States receive difference caps based on past spending levels, locking in funding disparities across the country well into the future. Past inefficiency and even waste is rewarded and efficiency is punished.
- The caps would be state-specific based on historic spending levels based on categories, such as senior citizens, people with disabilities, children, and adults.
- At least 200 different caps would be imposed by the federal government upon the states (50 states and D.C. times the different categories of enrollees).
- The cap would no longer adjust based on rising health care costs, new medical treatments, or surges in need (e.g., a recession or a pandemic).
- Once the cap is reached, states must make up the difference, cut services, or slash payments to providers.
This fundamentally changes Medicaid from a needs-based guarantee into a rationed, budget-limited program and from a federal-state partnership focused on providing care and services to one focused on bureaucracy, rules, regulations, auditors, lawyers, and accountants.
What Does That Mean for Kids?
As an example, suppose the federal government arbitrarily caps the level of funding to the State of Texas at $3,000 per child ages 0-18.
Most babies in Texas are born in hospitals, and the cost of childbirth – by itself – exceeds $3,000 – before even factoring in well-baby visits, immunizations, or early developmental screenings.
A per capita cap would intentionally shortchange babies, creating a disturbing incentive for states to cut, ration, or delay services for newborns.
The consequences of such a policy are not abstract. Medicaid provides health coverage for 41% of babies, or 1.5 million births, across the country. States in which 45% or more births are covered by Medicaid, include Texas and Alabama, Arizona, D.C., Georgia, Louisiana, Mississippi, New Mexico, New York, Oklahoma, South Carolina, Tennessee, and West Virginia. Lots of red states in that group.

The perverse incentives to limit and restrict care and services to babies would be felt in hospitals, pediatrician offices, and homes across America:
- A premature baby in the NICU whose life-saving care could be cut short because state Medicaid funding runs out.
- A child with cancer who has life-saving medical treatments and therapies threatened due to rationing of care.
- A child with cerebral palsy who loses access to crucial therapies because reimbursement rates are slashed.
- A baby with asthma who faces months-long waitlists to see a doctor due to provider shortages.
· A baby born in intensive care could have their Medicaid coverage determination delayed due to technology- and bureaucracy-imposed algorithms with the purpose of reducing Medicaid’s exposure to the costs of covering babies.
Tragically, per capita caps create financial incentives for states to place babies, children with cancer, and children with special health care needs on the chopping block.
This debate is not just about budgets — it’s about whether we will stand up for the most vulnerable children in our country or allow their health and well-being to be sacrificed for political convenience or to facilitate tax cuts for corporations and America’s wealthiest citizens.
How a Per Capita Cap Imposes Particularly Harm to Children
Unlike adults, children’s healthcare needs evolve as they grow — newborns require intensive care, toddlers need vaccinations, school-aged children need developmental screenings, and teens require mental health support. Medicaid, in its current form, ensures that each stage of development is met with the right care.
A per capita cap would break this system, forcing states to prioritize budget constraints over children’s health, leading to:
- Fewer early interventions, resulting in lifelong consequences for kids with disabilities and chronic illnesses.
- Cuts to mental health services, which are already underfunded for children.
- Strains on pediatric care providers, who rely on Medicaid’s reimbursement to serve low-income kids.
But there’s an even more insidious consequence of per capita caps, which is that they force states to pit Medicaid populations against one another. Because per capita caps set different spending limits for different eligibility groups — children, adults, people with disabilities, and seniors — states will be forced to choose who gets cut the most.
Historically, children are the most vulnerable in these budget fights.
Sen. John Chafee (R-RI), one of the original architects of the Children’s Health Insurance Program (CHIP), warned back in 1996 that when Medicaid is squeezed, children are the first to be sacrificed. As Chafee said on the Senate floor:
As states are forced to ration finite resources under a block grant, governors and legislators would be forced to choose among three very compelling groups of beneficiaries.
Who are they? Children, the elderly, and the disabled. They are the groups that primarily they would have to choose amongst. Unfortunately, I suspect that children would be the ones that would lose out.
Frankly, everybody is a loser when caps are arbitrarily imposed, but Sen. Chafee proved to be a prophet when he said that children would disproportionately be “the ones that would lose out.”
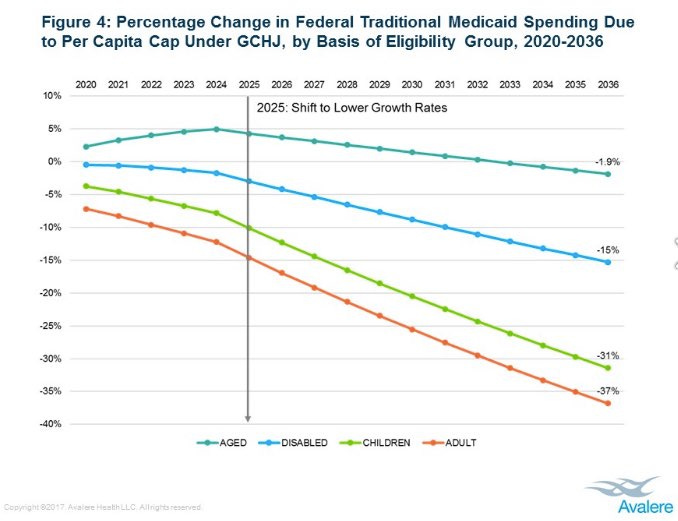
During the health care debates attempted to eliminate the Affordable Care Act (ACA) and to slash Medicaid, the House and Senate put forth proposals to cap Medicaid in ways that would have disproportionately cut funding for children. A study by Avalere Health found that children would suffer the steepest percentage reductions in funding over time – a 31% cut compared to 1.9% for seniors and 15% for people with disabilities – in the 2017 Graham-Cassidy Senate bill.
Why were children targeted the most? The reason is that children are politically voiceless — they don’t vote, they don’t have political action committees, and their needs are often overlooked in budget fights.
Fortunately, in 2017, Congress narrowly failed to impose these caps as part of ACA repeal efforts, thanks to overwhelming public opposition and Sen. John McCain’s (R-AZ) iconic “thumbs-down” moment in the Senate chambers.
Eight years later, the threat has returned, and children’s health is once again on the chopping block.
House leadership claims that the proposed $880 billion in cuts is just a number and not to worry. It’s not. It’s a direct attack on the health of millions of children.
Protect Child Health: At the Very Least, Do No Harm
This, however, is not an abstract, theoretical, or inconsequential debate. It is about real children and families and has real life-threatening consequences. When politicians talk about capping or cutting Medicaid, they are not just trimming a budget line – they are threatening the health, development, and future potential of nearly half of the nation’s children.
Consequently, to protect the health and well-being of millions of children, Congress must reject per capita caps or limits, and instead, work to strengthen Medicaid for the next generation.
At the very least, Congress should follow the Hippocratic Oath and “do no harm.”